 Currently, there are about a dozen systemic sclerosis patients on the pulsed plasma exchange (PPE) protocol described in this document: http://sclerodermainfo.org/pdf/TPE-Guidelines-US.pdf. Some have been on the protocol for years and others are just starting. I presented a research poster on four long-term patients with limited systemic sclerosis at a medical conference this past May. That is discussed in another post.
Currently, there are about a dozen systemic sclerosis patients on the pulsed plasma exchange (PPE) protocol described in this document: http://sclerodermainfo.org/pdf/TPE-Guidelines-US.pdf. Some have been on the protocol for years and others are just starting. I presented a research poster on four long-term patients with limited systemic sclerosis at a medical conference this past May. That is discussed in another post.
The purpose of this post is to document that PPE, like all treatment approaches used with systemic sclerosis (SSc) (with the exception of successful autologous stem cell transplants/HSCT), MUST be continued long term or any benefits seen from the treatment are likely to fade over time. SSc is a chronic disease and needs chronic treatment.
We now have two examples of what happens when PPE treatments are stopped (say, for a pandemic…). In the case of the first patient on PPE, a patient with centromere antibodies, the regular treatment protocol was stopped twice, once to see what would happen (done in 1996) and the other because of the pandemic (in 2020). There was also an experiment to see if the treatment gap could be lengthened beyond the normal eight-week interval. Here is a timeline for patient 1:
Patient 1
| 1985 | Initial symptom – Raynaud’s |
| 1985-1990 | Raynaud’s gradually worsens, puffy hands in morning, early GERD |
| January 1990 | Formally diagnosed with limited SSc with centromere antibodies |
| 1990-1993 | Symptoms steadily worsen with severe GERD and reduced lung functioning |
| Late 1993 | PPE treatments begin |
| Late 1994 | Major improvements in GERD and Raynaud’ symptoms |
| Late 1995 | GERD is completely gone, Raynaud’s almost completely gone |
| Summer 1996 | Treatment was stopped to see what would happen. Six months later, GERD was back |
| Early 1997 | Normal PPE treatment schedule resumes. GERD gradually improves and is gone after four treatment cycles |
| 1999-2001 | Inter-treatment interval slowly increased from 8 weeks to see if the gap could be increased. At a gap of 10 ½ weeks between treatment cycles, GERD returned and the normal 8-week gap was restarted. GERD is gone after three treatment cycles |
| 2020 | PPE treatments stopped because of COVID pandemic. As before, GERD starts to return at four months gap (versus normal 8-week gap). PPE resumes (patient wearing P99 protective gear). GERD gone after two treatment cycles. |
| Present | Normal 8-week schedule, no symptoms except for very mild Raynaud’s |
The second case is more interesting and more complex. This patient was diagnosed with early diffuse SSc with a rare antibody – U3-RNP. (The more common antibodies associated with a diagnosis of diffuse SSc are Scl-70 and RNA polymerase III.) As if often the case, initial symptoms with early diffuse SSc are often pain and fatigue, even before Raynaud’s and symptoms like GERD. In this case, the PPE protocol was interrupted by the pandemic also but had the added complication of a pregnancy. There is no published research data that I am aware of that documents the effects of pregnancy on therapeutic plasma exchange treatments.
I recently asked the patient who went through the PPE stoppage and pregnancy to send me an overview document on what has happened to date, including the COVID interruption and the pregnancy. Here is what was sent to me, unedited:
Patient 2:
| 2014 | First onset of symptoms in 2014. Symmetric pain in feet and hands. |
| 2015 | Rheumatologist prescribes Prednisone. Lab without identification of the related U3-RNP antibodies (they did not look for them). |
| 2016 | No diagnosis. Progressive symptom development. We treat it with Ibuprofen. Intermittent flare-ups with increased symptoms. |
| 2017 | Still symptoms; U3-RNP / Scleroderma diagnosis in August/September; Discovered Scleroderma Education Project/Ed/PPE |
| 2018 | First PPE treatment in February; Symptoms recede very quickly; 8 week intervals between PPEs; Mostly no symptoms. Very noticeable improvement to previous years. |
| 2019 | Continued PPE with 8-10 week intervals; Mostly no symptoms at all. Scleroderma is not a topic for us. Life is good. |
| 2020 | Last PPE session in January; Lockdowns/Pandemic/Travel Restrictions in Turkey; No PPE until July (6 month break). In the meanwhile, worsening symptoms. We’re controlling them with Ibuprofen; Restarting PPE in July with 8 week intervals; Pregnancy starts in October. Less symptoms during PPE, albeit short-lasting with only 1-2 weeks relief after 4th session. |
| 2021 | No Ibuprofen during pregnancy. Rather strong symptoms (pain) almost at pre PPE/2018 levels; Short-lasting relief during / after PPE sessions; June 2021. Baby is born; Symptoms treated with Ibuprofen; Maintaining 8 week intervals all year. |
| 2022 | We lower the intervals between sessions to five weeks after January 2022; Lung function and kidney tests etc. are all very good; Continuous improvement in pain symptoms; Since July 2022 mostly symptom free at 2018/2019 levels again; Increased intervals to 8 weeks between PPE. |
Discussion
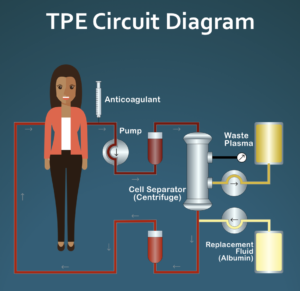
PPE is a treatment that targets the earliest stages of symptom development – reducing or stopping the endothelium damage that is considered to be the earliest functional stage of the disease process, long before any fibrotic damage occurs. Our working hypothesis for how PPE works is that each four-week treatment cycle eliminates the abnormal blood rheology that is characteristic of SSc: increased overall blood viscosity (thickness) caused by small groups of tightly clumped red blood cells. After the fourth weekly treatment, research documents that blood becomes normal, but slowly returns to pre-PPE levels over the next several months.
Normally, the eight-week treatment gap seems to be adequate to maintain any improvements seen from PPE. But when the normal protocol is stopped for four months or longer, blood has returned to baseline abnormal status and endothelium damage resumes, leading to return of symptoms.
After PPE was resumed for Patient 1 back in early 1997, the original 8-week treatment gap was used. More recently, we are starting to initially use a shorter gap than eight weeks to accelerate recovery. Once symptoms levels are back to PPE normal, we then can return to the normal eight-week gap to maintain these improvements.
Two patients are a very small sample size, of course, but the observed sequence of events are exactly what is predicted by the PPE treatment model. Bottom line is this: if PPE leads to symptom improvements, it is critical to continue these treatments indefinitely or symptoms will return. But the good news is that it appears to be the case that returning the normal PPE treatment protocol (or a slightly more aggressive temporary protocol) will again lead to the symptom improvements seen when PPE is successful initially.
Ed Harris
Founder/CEO
Of course. Eharris@sclerodermainfo.org
Could I communicate with you more directly via email or phone?
The second patient lived in Europe and paid out of pocket for treatments in Turkey at a Johns Hopkins affiliated hospital. I have a couple of potential researchers interested in being involved in a clinical trial, but the issue is getting funding. I am trying a couple of potential sources over the next few weeks.
Hi Ed,
Out of curiousity, how did the second patient manage to get treatment? I have recently had a drop in my DCLO function and am at a loss on how to pursue treatment. I had COVID in July 2022 and in Aug 2022 my yearly bloodwork showed a huge jump in my ANA. Have any clinical studies related to TPE treatment been started recently?